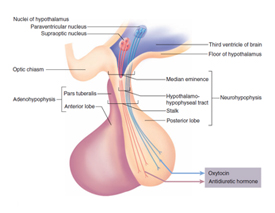
 Anatomy of the Pituitary Gland: The pituitary gland is a small piece of tissue of dual origin (pharynx for the adenohypophysis and brain for the neurohypophysis) attached to the brain by a stalk. The pituitary gland hangs downward from the brain and dwells in a small cavity known as the sella. The shape of the cavity containing the pituitary gland mimics a Turkish horse saddle (Sella Tursica). The gland is located at the center of the head at the juncture between the cranial cavity and nasal cavity. Embryonically, it is formed partly from the brain tissue itself (posterior lobe) and partly the throat tissue (anterior lobe). Once they are joined together during the developmental stage in a fetus, it forms the pituitary gland as a whole. The cherry-shaped pituitary gland is attached by a stalk (pituitary stalk) to the base of the brain, the hypothalamus. The posterior lobe, also known as the neurohypophysis, is directly connected to the hypothalamus by the pituitary stalk.
Anatomy of the Pituitary Gland: The pituitary gland is a small piece of tissue of dual origin (pharynx for the adenohypophysis and brain for the neurohypophysis) attached to the brain by a stalk. The pituitary gland hangs downward from the brain and dwells in a small cavity known as the sella. The shape of the cavity containing the pituitary gland mimics a Turkish horse saddle (Sella Tursica). The gland is located at the center of the head at the juncture between the cranial cavity and nasal cavity. Embryonically, it is formed partly from the brain tissue itself (posterior lobe) and partly the throat tissue (anterior lobe). Once they are joined together during the developmental stage in a fetus, it forms the pituitary gland as a whole. The cherry-shaped pituitary gland is attached by a stalk (pituitary stalk) to the base of the brain, the hypothalamus. The posterior lobe, also known as the neurohypophysis, is directly connected to the hypothalamus by the pituitary stalk.
Just above the pituitary gland lie the continuous visual nerve cables such as the right and left optic nerves, the optic chiasm which are the conjoined crossing cables, and the optic tracts which are the visual nerve cables conducting visual impulses to the brain. Just above the visual system is the hypothalamus, which is the vital brain tissue controlling homeostasis (maintenance of equilibrium-like conditions such as temperature and other parts of the autonomic nervous system, appetite, etc.) and instincts of the human body.
Pituitary Tumors: Many types of tumors can occur in the pituitary gland. The most common tumors in the pituitary gland are pituitary adenomas (which are benign). However, metastatic cancer can dwell in the pituitary gland when the cancer cells metastasize to the pituitary gland.
Benign Pituitary Adenomas: can be divided into nonfunctioning tumors and functioning tumors depending on the capability of tumor cells to produce hormones.
Nonfunctioning: Pituitary adenomas do not produce active hormones by themselves. Nonfunctioning tumors mechanically compress surrounding structures such as normal pituitary gland and optic system.
Functioning: Pituitary adenomas produce a hormone(s) in excess. Excess amount of hormone produced by tumor cells cause symptoms dependent on the type of hormone. Functioning pituitary adenomas include prolactinomas (PRL overproduction), adenomas that cause Cushing's disease (ACTH overproduction), adenomas that cause gigantism or acromegaly (GH overproduction), and TSH-producing tumors.
Prolactinomas: are the most common functioning pituitary adenomas and produce excess amount of prolactin that results in amenorrhea (irregular menstrual periods), breast discharge (galactorrhea), infertility, and sexual dysfunction. Pituitary adenomas that produce ACTH cause.
Cushing's Disease: Symptoms of Cushing's disease include ruddy moon face, truncal obesity, buffalo hump, hypertension, abdominal striae, easy bruisability, depression, psychosis, irregular menses, impotence, osteoporosis, muscle weakness, etc. Cushing's disease is a serious condition requiring prompt treatments. Pituitary adenomas that produce growth hormone cause
Gigantism: in children (due to still active growth plates)
Acromegaly: in adults. In acromegaly the jaw, cheeks, fingers, and toes are thickened along with the enlargement of soft tissues such as the tongue, nose, and lips. Affected adult patients might find that their shoes or hats do not fit properly any longer. TSH-producing adenomas, which are relatively rare, cause
Goiters: (enlarged thyroid gland) and thyroid hyper-function disorders.
Symptoms of Pituitary Tumors
Symptoms of pituitary tumors are: 1) , 2) , 3) , 4)
- Hormonal disorders from excessive production of hormones from the tumors
- Pituitary hormonal dysfunction from compression of the normal pituitary tissue
- Visual disorders from tumor compression of the optic system
- Other symptoms related to the compression of the surrounding brain such as the hypothalamus.
 When functioning pituitary adenomas produce hormones, the excess amount of hormone will cause particular hormonal disorder symptoms depending on the type of hormone as described earlier. When pituitary adenomas become large, they compress and make the normal pituitary gland tissue hypo- or non-functional (hypopituitarism) resulting in pituitary hormonal dysfunction. Most often, nonfunctioning adenomas grow to large sizes undetected and result in hypopituitarism. However, functioning adenomas can also cause general hypopituitarism even while producing an excess amount of a particular hormone.
When pituitary tumors compress the optic system (which is located just above the pituitary gland), visual disorders may develop. The most common visual disorder is a visual field defect at the outside view of each eye known as bitemporal hemianopsia.
Other symptoms such as memory disorder, hydrocephalus, and other brain dysfunction can develop if the tumor is large enough to compress the hypothalamus. Pituitary adenomas are known to bleed spontaneously (pituitary apoplexy). When spontaneous bleeding occurs inside a pituitary adenoma, symptoms of severe headaches, visual disorders, eye movement disorder, and altered consciousness can develop. Immediate medical treatment is necessary and surgical treatment is often required.
When functioning pituitary adenomas produce hormones, the excess amount of hormone will cause particular hormonal disorder symptoms depending on the type of hormone as described earlier. When pituitary adenomas become large, they compress and make the normal pituitary gland tissue hypo- or non-functional (hypopituitarism) resulting in pituitary hormonal dysfunction. Most often, nonfunctioning adenomas grow to large sizes undetected and result in hypopituitarism. However, functioning adenomas can also cause general hypopituitarism even while producing an excess amount of a particular hormone.
When pituitary tumors compress the optic system (which is located just above the pituitary gland), visual disorders may develop. The most common visual disorder is a visual field defect at the outside view of each eye known as bitemporal hemianopsia.
Other symptoms such as memory disorder, hydrocephalus, and other brain dysfunction can develop if the tumor is large enough to compress the hypothalamus. Pituitary adenomas are known to bleed spontaneously (pituitary apoplexy). When spontaneous bleeding occurs inside a pituitary adenoma, symptoms of severe headaches, visual disorders, eye movement disorder, and altered consciousness can develop. Immediate medical treatment is necessary and surgical treatment is often required.
 Treatments of Pituitary Tumors
Treatments of Pituitary Tumors
Medical, surgical, and/or radiation treatments are available for pituitary tumors. Prolactinomas can be treated with medications (bromocriptine is most commonly used). Surgical treatment is indicated when medication side effects or intolerance develops. Acromegaly can be treated with octreotide medication but does not respond as well as prolactinomas do with bromocriptine. Often, acromegaly requires surgical removal of the tumor. If surgery is not successful, octreotide medication or radiation treatment (gamma-knife surgery) can be considered. Cushing's disease requires surgical removal of the tumor as the first line of treatment. If surgical treatments fails to relieve symptoms, radiosurgery or medical treatments can be instituted. TSH-secreting adenomas require surgical treatment. When nonfunctioning tumors cause symptoms, surgical treatment is the first choice among the treatments. If surgical treatments are not successful, radiation treatment (conventional radiation or radiosurgery) has to be considered. Endoscopic Pituitary Surgery is performed through a natural nasal air pathway without any incisions (unlike the conventional microscopic surgery performed with an incision made under the upper lip or inner aspect of a nostril). Endoscopic surgery does not require the use of a metallic transsphenoidal retractor that is used for conventional microscopic surgery. A 4-mm endoscope is placed in front of the tumor in the sphenoidal sinus and the tumor is removed with specially designed surgical tools. Conventional transsphenoidal surgery is performed under the operating microscope via an incision underneath the upper lip (sublabial incision) or intranasal incision (transfixional incision). It requires two to three days of nasal packing and three to five days of hospital stay.
Copyright © 2015 Dr. Gopal Achary. All rights reserved.
Site Designed & Maintained by Rushi Web World
Site Designed & Maintained by Rushi Web World