 Acoustic neuromas are benign brain tumors usually arising from the vestibular nerve (balance nerve), most commonly from the superior vestibular nerve. Sound travels through the ear drum to the middle ear and enters into the inner ear organ. Sound is converted to nerve impulses, and the nerve impulses travel through the hearing nerve (cochlear nerve) to the brain. The inner ear organ has a balance organ in addition to a hearing organ. This balance organ system is extended to the brain via two nerve cables named the superior vestibular nerve and inferior vestibular nerve. The facial nerve also travels together towards the brain.
Acoustic neuromas are benign brain tumors usually arising from the vestibular nerve (balance nerve), most commonly from the superior vestibular nerve. Sound travels through the ear drum to the middle ear and enters into the inner ear organ. Sound is converted to nerve impulses, and the nerve impulses travel through the hearing nerve (cochlear nerve) to the brain. The inner ear organ has a balance organ in addition to a hearing organ. This balance organ system is extended to the brain via two nerve cables named the superior vestibular nerve and inferior vestibular nerve. The facial nerve also travels together towards the brain.
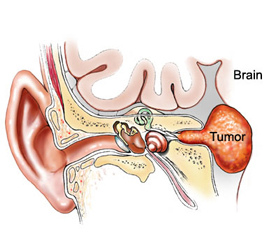
The cochlear nerve, the two vestibular nerves (superior and inferior), and facial nerve travel together in the inner ear canal to enter into the brain. When an acoustic tumor develops, it most often develops at the superior vestibular nerve in the inner ear canal (internal acoustic canal). Thus, the tumor compresses the hearing nerve (cochlear nerve) causing tinnitus and hearing impairment. It can also cause dizziness or vertigo by balance nerve dysfunction. The facial nerve tolerates compression better than the other nerves so that facial weakness develops very late.
Although hearing tests are required for hearing evaluation in aiding the diagnosis, definitive diagnosis of an acoustic neuroma is made with MR scans of the brain. Treatments for acoustic neuromas consist of observation with interval MR scans, surgical removal, or radiosurgery.
Large tumors generally require surgical removal, while small tumors also have the option of radiosurgery treatment. Microsurgical removal of a small tumor can achieve a 90-99% chance of normal facial function and a 60-80% chance of hearing preservation postoperatively. Large tumors carry higher chances of temporary facial weakness and hearing loss postoperatively. Retromastoid or Retrosigmoid Approach for acoustic tumor surgery because it results in high probability of the preservation of the facial nerve and hearing nerve functions. A retromastoid approach is made with an approximately one-inch (or three-cm) skull opening via a two-inch (or five-cm) skin incision behind the ear. Hearing and facial nerve functions are continually monitored electrophysiologically throughout the operation. The operating microscope and an endoscope are used for surgical visualization and the tumor is excised with delicate microdissection.
Copyright © 2015 Dr. Gopal Achary. All rights reserved.
Site Designed & Maintained by Rushi Web World
Site Designed & Maintained by Rushi Web World