Pituitary Tumors : Pituitary tumors are abnormal growths that develop in your pituitary gland. Some pituitary tumors cause excessive production of hormones that regulate important functions of your body. Other pituitary tumors can restrict normal functions of your pituitary gland, causing it to produce lower levels of hormones.
Acoustic Neuromas : An acoustic neuroma is a noncancerous growth that develops on the eighth cranial nerve. Also known as the vestibulocochlear nerve, it connects the inner ear with the brain and has two different parts.
Meningiomas : Meningiomas are a diverse set of tumors arising from the meninges, the membranous layers surrounding the central nervous system. They arise from the arachnoid "cap" cells of the arachnoid villi in the meninges. These tumors usually are benign in nature; however, a small percentage are malignant.
Craniopharyngiomas : Craniopharyngioma is a type of brain tumor derived from pituitary gland embryonic tissue, that occurs most commonly in children but also in men and women in their 50s and 60s. People may present with bitemporal inferior quadrantanopia leading to bitemporal hemianopia, as the tumor may compress the optic chiasm.
Pineal Tumors : These tumors originate from normal cells in the pineal gland. The pineal gland is located in the center of the brain and is involved in the secretion of specific hormones. Tumor types occurring in the pineal region may or may not involve the pineal gland. True pineal cell tumors—pineocytoma, pineoblastoma, and mixed pineal tumors—are covered on this page. Tumors that may occur in this region but are not necessarily pineal tumors include: germinoma, non-germinoma (eg, teratoma, endodermal sinus tumor, embryonal cell tumor, choriocarcinoma, and mixed tumors), meningioma, astrocytoma, ganglioglioma, and dermoid cysts. Information on these particular tumors can be found elsewhere on this site.
Skull Base Tumor : The skull base is the area behind the eyes and nose that slopes down to the back of the head. It forms the floor, or base, of the skull. The spinal cord, multiple nerves and the major blood vessels of the brain, head and neck pass through openings in the skull base. The term "skull base tumor" refers to the tumor's location. The type of cancer cell can be one of several. Some are malignant (cancer), and some are benign (non-cancerous). Even benign tumors can cause problems because they are growing in a confined space. Skull Base Tumor Types: Skull base tumors are grouped by location and the type of cells in the tumor. Where a skull base tumor begins can make a difference in the type of cancer cells. Location also can influence symptoms and treatment.
Chordoma : Chordoma is a rare slow-growing neoplasm thought to arise from cellular remnants of the notochord. The evidence for this is the location of the tumors (along the neuraxis), the similar immunohistochemical staining patterns, and the demonstration that notochordal cells are preferentially left behind in the clivus and sacrococcygeal regions when the remainder of the notochord regresses during fetal life.
Arachnoid Cysts : Arachnoid cysts are cerebrospinal fluid covered by arachnoidal cells and collagen that may develop between the surface of the brain and the cranial base or on the arachnoid membrane, one of the three membranes that cover the brain and the spinal cord.
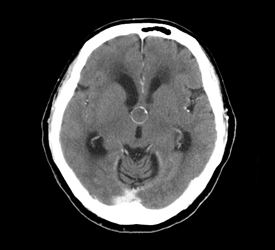 Colloid Cysts : A colloid cyst is a cyst containing gelatinous material in the brain. It is almost always found just posterior to the foramen of Monro in the anterior aspect of the third ventricle, originating from the roof of the ventricle. Because of its location, it can cause obstructive hydrocephalus and increased intracranial pressure. A Colloid cyst of the third ventricle accounts for 0.55 to 2 percent of all intracranial tumors, about one per 1000 in asymptomatic patients
Colloid Cysts : A colloid cyst is a cyst containing gelatinous material in the brain. It is almost always found just posterior to the foramen of Monro in the anterior aspect of the third ventricle, originating from the roof of the ventricle. Because of its location, it can cause obstructive hydrocephalus and increased intracranial pressure. A Colloid cyst of the third ventricle accounts for 0.55 to 2 percent of all intracranial tumors, about one per 1000 in asymptomatic patients
Symptoms can include headache, vertigo, memory deficits, diplopia, behavioral disturbances and in extreme cases, sudden death. Untreated pressure caused by these cysts can result in brain herniation. Colloid cyst symptoms have been associated with 4 variables: cyst size, cyst imaging characteristics, ventricular size, and patient age. The developmental origin is unclear, though they may be of endodermal origin, which would explain the mucin-producing, ciliated cell type. These cysts can be surgically resected, and opinion is divided about the advisability of this.
 Hydrocephalus : Hydrocephalus is a medical condition in which there is an abnormal accumulation of cerebrospinal fluid (CSF) in the brain. This causes increased intracranial pressure inside the skull and may cause progressive enlargement of the head if it occurs in childhood, potentially causing convulsion, tunnel vision, and mental disability. It was once informally called "Water on the brain."
Hydrocephalus : Hydrocephalus is a medical condition in which there is an abnormal accumulation of cerebrospinal fluid (CSF) in the brain. This causes increased intracranial pressure inside the skull and may cause progressive enlargement of the head if it occurs in childhood, potentially causing convulsion, tunnel vision, and mental disability. It was once informally called "Water on the brain."
Hydrocephalus can be caused by congenital or acquired factors. Congenital causes include Spina Bifida, Arnold–Chiari malformation, craniosynostosis, Dandy–Walker syndrome, and Vein of Galen malformations. Acquired causes include hemorrhage, meningitis, head trauma, tumors, and cysts.
Two types of hydrocephalus are commonly described non-communicating hydrocephalus and communicating hydrocephalus, although there is evidence that communicating forms can lead to obstruction of CSF flow in many instances.
In non-communicating hydrocephalus, the CSF in the ventricles can not reach the subarachnoid space. This results from obstruction of interventricular foramina, cerebral aqueduct, or the outflow foramens of the fourth ventricle (median and lateral apertures). The most common obstruction is in the cerebral aqueduct. A block at any of these sites leads rapidly to dilatation of one or more ventricles. If the skull is still pliable, as it is in children younger than 2 years, the head may enlarge.
In communicating hydrocephalus, the obstruction of CSF flow is in the subarachnoid space from prior bleeding or meningitis. This causes thickening of the arachnoid leading to blockage of the return-flow channels. In some patients, the spaces filled by CSF are uniformly enlarged without an increase in intercranial pressure. This special form of communicating hydrocephalus is called normal pressure hydrocephalus (NPH), which results specifically from impaired CSF reabsorption at the arachnoid granulations. NPH's clinical manifestations are gait abnormality, dementia, and involuntary urination. NPH usually occurs in elderly patients.
Trigeminal Neuralgia : Trigeminal neuralgia (TN or TGN), also known as prosopalgia, or Fothergill's disease is a neuropathic disorder characterized by episodes of intense pain in the face, originating from the trigeminal nerve. The clinical association between TN and hemifacial spasm is the so-called tic douloureux. It has been described as among the most painful conditions known to humankind. It is estimated that 1 in 15,000 or 20,000 people suffer from TN, although the actual figure may be significantly higher due to frequent misdiagnosis. In most cases, TN symptoms begin appearing more frequently over the age of 50, although there have been cases with patients being as young as three years of age. It is more common in females than males.
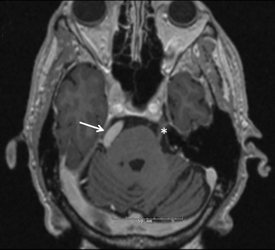 Hemifacial Spasm : Hemifacial spasm is a neuromuscular disorder characterized by frequent involuntary contractions (spasms) of the muscles on one side (hemi-) of the face (facial). The disorder occurs in both men and women, although it more frequently affects middle-aged or elderly women. It is much more common in the Asian population. The first symptom is usually an intermittent twitching of the eyelid muscle that can lead to forced closure of the eye. The spasm may then gradually spread to involve the muscles of the lower face, which may cause the mouth to be pulled to one side. Eventually the spasms involve all of the muscles on one side of the face almost continuously. The condition may be caused by a facial nerve injury, or a tumor, or it may have no apparent cause. Rarely, doctors see individuals with spasm on both sides of the face. Most often hemifacial spasm is caused by a blood vessel pressing on the facial nerve at the place where it exits the brainstem.
Hemifacial Spasm : Hemifacial spasm is a neuromuscular disorder characterized by frequent involuntary contractions (spasms) of the muscles on one side (hemi-) of the face (facial). The disorder occurs in both men and women, although it more frequently affects middle-aged or elderly women. It is much more common in the Asian population. The first symptom is usually an intermittent twitching of the eyelid muscle that can lead to forced closure of the eye. The spasm may then gradually spread to involve the muscles of the lower face, which may cause the mouth to be pulled to one side. Eventually the spasms involve all of the muscles on one side of the face almost continuously. The condition may be caused by a facial nerve injury, or a tumor, or it may have no apparent cause. Rarely, doctors see individuals with spasm on both sides of the face. Most often hemifacial spasm is caused by a blood vessel pressing on the facial nerve at the place where it exits the brainstem.
Is there any treatment?
Surgical treatment in the form of microvascular decompression, which relieves pressure on the facial nerve, will relieve hemifacial spasm in many cases. This intervention has significant potential side-effects, so risks and benefits have to be carefully balanced. Other treatments include injections of botulinum toxin into the affected areas, which is the most effective therapy and the only one used in most cases. Drug therapy is generally not effective.
Arteriovenous Malformation : Arteriovenous malformation (AVM) is an abnormal connection between arteries and veins, bypassing the capillary system. This vascular anomaly is widely known because of its occurrence in the central nervous system, but can appear in any location. Although many AVMs are asymptomatic, they can cause intense pain or bleeding or lead to other serious medical problems.
AVMs are usually congenital and belong to the RASopathies. The genetic transmission patterns of AVM, if any, are unknown. AVM is not generally thought to be an inherited disorder, unless in the context of a specific hereditary syndrome.
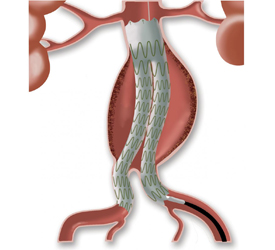 Aneurysms : An aneurysm or aneurism is a localized, blood-filled balloon-like bulge in the wall of a blood vessel.
Aneurysms : An aneurysm or aneurism is a localized, blood-filled balloon-like bulge in the wall of a blood vessel.
Aneurysms can occur in any blood vessel, with examples including aneurysms of the circle of Willis in the brain, aortic aneurysms affecting the thoracic aorta, and abdominal aortic aneurysms. Aneurysms can also occur within the heart itself.
As an aneurysm increases in size, the risk of rupture increases. A ruptured aneurysm can lead to bleeding and subsequent hypovolemnealic shock, leading to death. Aneurysms are a result of a weakened blood vessel wall, and can be a result of a hereditary condition or an acquired disease. Aneurysms can also be a nidus for clot formation (thrombosis) and embolization.
Acoustic Neuromas : An acoustic neuroma is a noncancerous growth that develops on the eighth cranial nerve. Also known as the vestibulocochlear nerve, it connects the inner ear with the brain and has two different parts.
Meningiomas : Meningiomas are a diverse set of tumors arising from the meninges, the membranous layers surrounding the central nervous system. They arise from the arachnoid "cap" cells of the arachnoid villi in the meninges. These tumors usually are benign in nature; however, a small percentage are malignant.
Craniopharyngiomas : Craniopharyngioma is a type of brain tumor derived from pituitary gland embryonic tissue, that occurs most commonly in children but also in men and women in their 50s and 60s. People may present with bitemporal inferior quadrantanopia leading to bitemporal hemianopia, as the tumor may compress the optic chiasm.
Pineal Tumors : These tumors originate from normal cells in the pineal gland. The pineal gland is located in the center of the brain and is involved in the secretion of specific hormones. Tumor types occurring in the pineal region may or may not involve the pineal gland. True pineal cell tumors—pineocytoma, pineoblastoma, and mixed pineal tumors—are covered on this page. Tumors that may occur in this region but are not necessarily pineal tumors include: germinoma, non-germinoma (eg, teratoma, endodermal sinus tumor, embryonal cell tumor, choriocarcinoma, and mixed tumors), meningioma, astrocytoma, ganglioglioma, and dermoid cysts. Information on these particular tumors can be found elsewhere on this site.
Skull Base Tumor : The skull base is the area behind the eyes and nose that slopes down to the back of the head. It forms the floor, or base, of the skull. The spinal cord, multiple nerves and the major blood vessels of the brain, head and neck pass through openings in the skull base. The term "skull base tumor" refers to the tumor's location. The type of cancer cell can be one of several. Some are malignant (cancer), and some are benign (non-cancerous). Even benign tumors can cause problems because they are growing in a confined space. Skull Base Tumor Types: Skull base tumors are grouped by location and the type of cells in the tumor. Where a skull base tumor begins can make a difference in the type of cancer cells. Location also can influence symptoms and treatment.
Chordoma : Chordoma is a rare slow-growing neoplasm thought to arise from cellular remnants of the notochord. The evidence for this is the location of the tumors (along the neuraxis), the similar immunohistochemical staining patterns, and the demonstration that notochordal cells are preferentially left behind in the clivus and sacrococcygeal regions when the remainder of the notochord regresses during fetal life.
Arachnoid Cysts : Arachnoid cysts are cerebrospinal fluid covered by arachnoidal cells and collagen that may develop between the surface of the brain and the cranial base or on the arachnoid membrane, one of the three membranes that cover the brain and the spinal cord.
Colloid Cysts : A colloid cyst is a cyst containing gelatinous material in the brain. It is almost always found just posterior to the foramen of Monro in the anterior aspect of the third ventricle, originating from the roof of the ventricle. Because of its location, it can cause obstructive hydrocephalus and increased intracranial pressure. A Colloid cyst of the third ventricle accounts for 0.55 to 2 percent of all intracranial tumors, about one per 1000 in asymptomatic patients
Symptoms can include headache, vertigo, memory deficits, diplopia, behavioral disturbances and in extreme cases, sudden death. Untreated pressure caused by these cysts can result in brain herniation. Colloid cyst symptoms have been associated with 4 variables: cyst size, cyst imaging characteristics, ventricular size, and patient age. The developmental origin is unclear, though they may be of endodermal origin, which would explain the mucin-producing, ciliated cell type. These cysts can be surgically resected, and opinion is divided about the advisability of this.
Hydrocephalus : Hydrocephalus is a medical condition in which there is an abnormal accumulation of cerebrospinal fluid (CSF) in the brain. This causes increased intracranial pressure inside the skull and may cause progressive enlargement of the head if it occurs in childhood, potentially causing convulsion, tunnel vision, and mental disability. It was once informally called "Water on the brain."
Hydrocephalus can be caused by congenital or acquired factors. Congenital causes include Spina Bifida, Arnold–Chiari malformation, craniosynostosis, Dandy–Walker syndrome, and Vein of Galen malformations. Acquired causes include hemorrhage, meningitis, head trauma, tumors, and cysts.
Two types of hydrocephalus are commonly described non-communicating hydrocephalus and communicating hydrocephalus, although there is evidence that communicating forms can lead to obstruction of CSF flow in many instances.
In non-communicating hydrocephalus, the CSF in the ventricles can not reach the subarachnoid space. This results from obstruction of interventricular foramina, cerebral aqueduct, or the outflow foramens of the fourth ventricle (median and lateral apertures). The most common obstruction is in the cerebral aqueduct. A block at any of these sites leads rapidly to dilatation of one or more ventricles. If the skull is still pliable, as it is in children younger than 2 years, the head may enlarge.
In communicating hydrocephalus, the obstruction of CSF flow is in the subarachnoid space from prior bleeding or meningitis. This causes thickening of the arachnoid leading to blockage of the return-flow channels. In some patients, the spaces filled by CSF are uniformly enlarged without an increase in intercranial pressure. This special form of communicating hydrocephalus is called normal pressure hydrocephalus (NPH), which results specifically from impaired CSF reabsorption at the arachnoid granulations. NPH's clinical manifestations are gait abnormality, dementia, and involuntary urination. NPH usually occurs in elderly patients.
Trigeminal Neuralgia : Trigeminal neuralgia (TN or TGN), also known as prosopalgia, or Fothergill's disease is a neuropathic disorder characterized by episodes of intense pain in the face, originating from the trigeminal nerve. The clinical association between TN and hemifacial spasm is the so-called tic douloureux. It has been described as among the most painful conditions known to humankind. It is estimated that 1 in 15,000 or 20,000 people suffer from TN, although the actual figure may be significantly higher due to frequent misdiagnosis. In most cases, TN symptoms begin appearing more frequently over the age of 50, although there have been cases with patients being as young as three years of age. It is more common in females than males.
Hemifacial Spasm : Hemifacial spasm is a neuromuscular disorder characterized by frequent involuntary contractions (spasms) of the muscles on one side (hemi-) of the face (facial). The disorder occurs in both men and women, although it more frequently affects middle-aged or elderly women. It is much more common in the Asian population. The first symptom is usually an intermittent twitching of the eyelid muscle that can lead to forced closure of the eye. The spasm may then gradually spread to involve the muscles of the lower face, which may cause the mouth to be pulled to one side. Eventually the spasms involve all of the muscles on one side of the face almost continuously. The condition may be caused by a facial nerve injury, or a tumor, or it may have no apparent cause. Rarely, doctors see individuals with spasm on both sides of the face. Most often hemifacial spasm is caused by a blood vessel pressing on the facial nerve at the place where it exits the brainstem.
Is there any treatment?
Surgical treatment in the form of microvascular decompression, which relieves pressure on the facial nerve, will relieve hemifacial spasm in many cases. This intervention has significant potential side-effects, so risks and benefits have to be carefully balanced. Other treatments include injections of botulinum toxin into the affected areas, which is the most effective therapy and the only one used in most cases. Drug therapy is generally not effective.
Arteriovenous Malformation : Arteriovenous malformation (AVM) is an abnormal connection between arteries and veins, bypassing the capillary system. This vascular anomaly is widely known because of its occurrence in the central nervous system, but can appear in any location. Although many AVMs are asymptomatic, they can cause intense pain or bleeding or lead to other serious medical problems.
AVMs are usually congenital and belong to the RASopathies. The genetic transmission patterns of AVM, if any, are unknown. AVM is not generally thought to be an inherited disorder, unless in the context of a specific hereditary syndrome.
Aneurysms : An aneurysm or aneurism is a localized, blood-filled balloon-like bulge in the wall of a blood vessel.
Aneurysms can occur in any blood vessel, with examples including aneurysms of the circle of Willis in the brain, aortic aneurysms affecting the thoracic aorta, and abdominal aortic aneurysms. Aneurysms can also occur within the heart itself.
As an aneurysm increases in size, the risk of rupture increases. A ruptured aneurysm can lead to bleeding and subsequent hypovolemnealic shock, leading to death. Aneurysms are a result of a weakened blood vessel wall, and can be a result of a hereditary condition or an acquired disease. Aneurysms can also be a nidus for clot formation (thrombosis) and embolization.
Copyright © 2015 Dr. Gopal Achary. All rights reserved.
Site Designed & Maintained by Rushi Web World
Site Designed & Maintained by Rushi Web World